+91-9866908086, +91-9494138086
Can Less ‘Sun-Time’ Drive High Blood Pressure?
The Sunshine Link: Is Vitamin D Deficiency the Hidden Driver of Hypertension?
Contents of This Post:
- The Biological Blueprint: How Vitamin D Talks to Your Arteries?
- What Do the Clinical Studies Actually Say? The Research Roundup
- When the Link is Strong: Subgroups Who Benefit Most
- The Grey Areas: Why Vitamin D Isn’t a “Magic Pill” for Everyone
- The “Difference” Factor: When Hypertension is NOT Linked to Vitamin D
- From Lab to Life: What Should You Do Next?
- Partner in Health: Help Us Bridge the Gap in Cardiac Care: Explore Pharma PCD Opportunities
Hypertension already places a significant burden on global health. As populations age and daily life becomes increasingly sedentary, more individuals are likely to develop high blood pressure over time. However, why are we discussing the ‘sunshine vitamin’ here? It may draw your attention. And you really need this one!
When you think of Vitamin D, your mind likely jumps to strong bones and calcium. Similarly, when you think of high blood pressure (hypertension, HTN), you probably think of heart, angina, salt, stress, lifestyle and hours spent on a treadmill. For a long time, medical science kept these two in separate boxes.
However, recent clinical research is blurring those lines.
Scientists are discovering that Vitamin D—the “sunshine vitamin”—does far more than just protect your skeleton. It appears to act as a silent regulator for your cardiovascular system. Furthermore, in a country like India, where nearly 70% to 90% of the population grapples with Vitamin D deficiency, and hypertension remains a leading cause of heart disease, this connection is more than just a scientific curiosity. It is a vital health lead.
But does a lack of sun exposure directly cause your blood pressure to spike? Or is the relationship more complex?
In this post, we dive into the latest research to uncover how these two “silent” conditions interact. We will break down the complex mechanics of how Vitamin D influences your blood vessels, examine what the clinical trials actually tell us, and—most importantly—help you understand if stepping into the sun (or reaching for a supplement) could be your heart’s secret weapon.
The Biological Blueprint: How Vitamin D “Talks” to Your Arteries?
Firstly, to understand why a vitamin usually associated with bone health affects your blood pressure, we have to look at Vitamin D as more than just a nutrient. In reality, Vitamin D acts as a pro-hormone. Once your body processes it, it begins communicating with almost every cell in your cardiovascular system, from the muscles in your heart to the delicate lining of your blood vessels.
The heart of this connection lies in a complex internal “regulatory thermostat” called the Renin-Angiotensin System (RAS). (Reference)
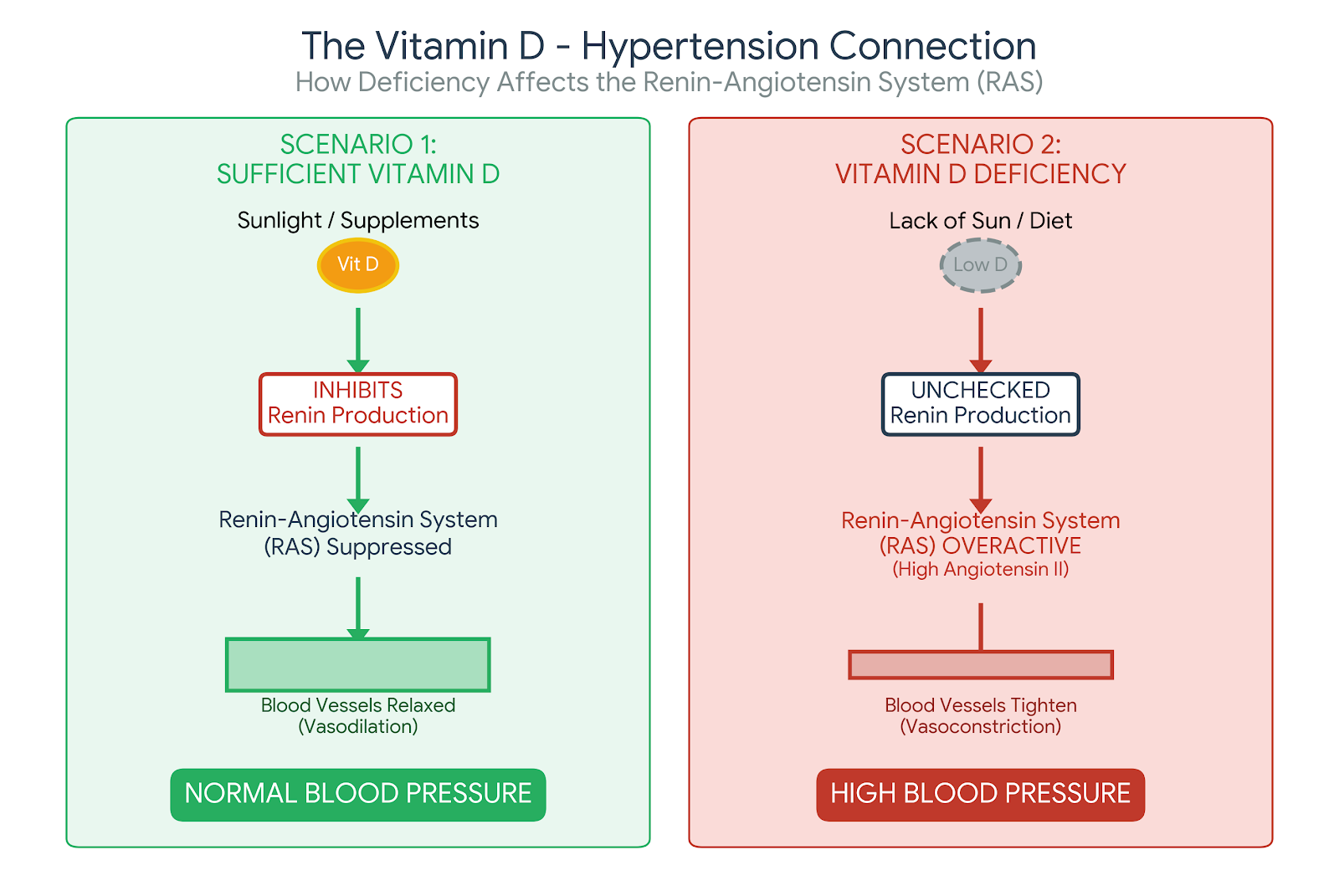
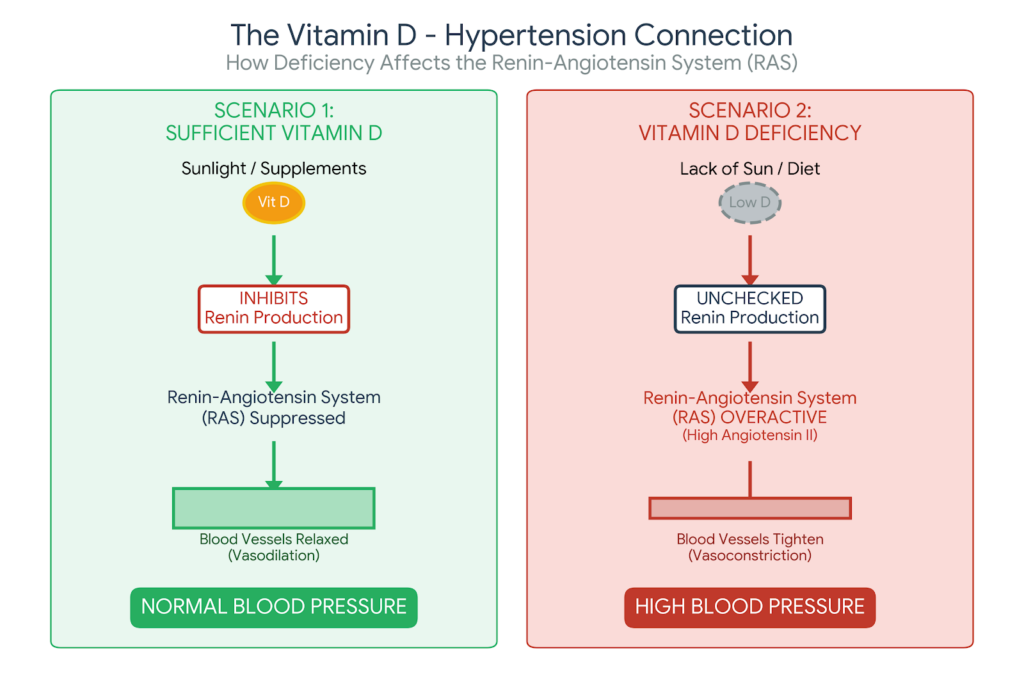
1. The RAS: Your Body’s Blood Pressure Thermostat Linked With Vitamin D
Your kidneys produce a hormone called Renin. Now, think of Renin as a signal that tells your body to tighten your blood vessels and hold onto salt and water. While this system is vital for keeping you alive if you’re dehydrated or bleeding, an overactive RAS is a leading driver of chronic hypertension.
Research, including landmark studies published in The Journal of Clinical Investigation, has shown that Vitamin D acts as a natural potent inhibitor of Renin [1]. When you have sufficient Vitamin D, it essentially tells your kidneys, “We have enough pressure; you can dial back the Renin production.” But without enough Vitamin D, this “off-switch” fails. So, the RAS runs wild, leading to constricted arteries and higher pressure.
2. The “Teflon” Lining of Your Arteries: Vitamin D & Nitric Oxide Link
Every blood vessel in your body is lined with a thin layer of cells called the endothelium. In a healthy person, this lining is like Teflon—smooth and flexible. It produces Nitric Oxide, a gas that tells your arteries to relax and widen (vasodilation). Clinical studies have identified Vitamin D Receptors (VDR) directly on these endothelial cells.
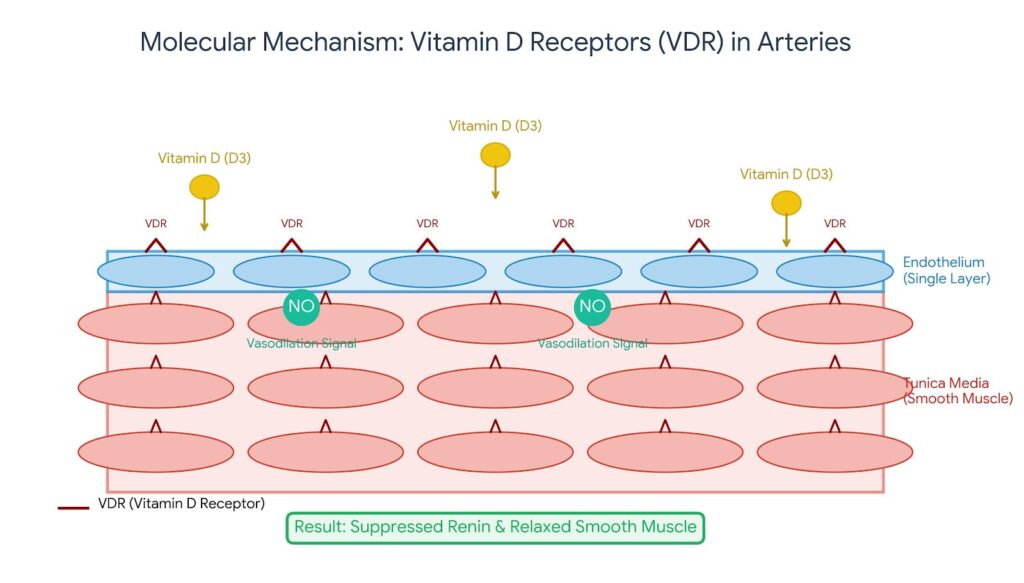
Also, research suggests that Vitamin D helps:
- Firstly, in boosting Nitric Oxide: This then increases the “relaxation signal” to your arteries [2].
- Secondly, in reducing oxidative stress: Vitamin D also mops up harmful molecules that “rust” your arteries, keeping them supple rather than stiff.
- Also, in lowering inflammation: Chronic inflammation makes blood vessels rigid; Vitamin D helps dampen the inflammatory response.
3. The Calcium Connection (The Delicate Balance)
You may be knowing that Vitamin D helps you absorb calcium. However, in the context of hypertension, Vitamin D also influences how calcium moves within the smooth muscle cells of your blood vessel walls. So, by regulating these calcium channels, Vitamin D helps prevent the muscle cells in your arteries from contracting too tightly, which would otherwise narrow the “pipes” and skyrocket your blood pressure.
What the Research Says?
Large-scale observational studies—such as those following thousands of participants over decades—frequently show an inverse relationship: as Vitamin D levels go down, blood pressure readings tend to go up. For example, data from the Third National Health and Nutrition Examination Survey (NHANES III) highlighted that individuals in the highest quartile of Vitamin D levels had significantly lower systolic blood pressure than those in the lowest [3].
So, think of Vitamin D as the “manager” of your blood pressure system. It keeps your arteries relaxed, prevents your kidneys from over-pressurising the “pipes,” and protects the lining of your heart. When the manager is missing (deficiency), the system becomes inefficient, stiff, and high-pressure.
The Research Roundup: What Do the Clinical Studies Actually Say?
If the biological connection between Vitamin D and blood pressure is so clear, you might wonder why every doctor doesn’t simply prescribe a supplement the moment a patient’s blood pressure creeps up. The truth lies in the “Research Gap”—the difference between what we see in a lab and what happens in a wide-scale human population.
Now, to understand the evidence, we have to look at two different types of research: Observational Studies and Randomised Controlled Trials (RCTs).
1. The Strong Link: Observational Evidence
Firstly, observational studies look at large groups of people over time. Besides, these studies are remarkably consistent. Research involving tens of thousands of participants, such as the Framingham Offspring Study, has repeatedly shown that people with low Vitamin D levels have a significantly higher risk of developing hypertension later in life. According to the study, individuals with Vitamin D deficiency had a 62% higher risk of a cardiovascular event compared to those with normal levels [4].
In addition, a massive genetic study involving over 140,000 individuals (using a technique called Mendelian Randomisation) concluded that for every 10% increase in Vitamin D levels, there was an associated 8% decrease in the risk of developing hypertension [5].
2. The Mixed Results: Randomised Controlled Trials (RCTs)
This is where the “Grey Areas” begin. In an RCT, one group gets Vitamin D, and the other gets a placebo. Surprisingly, when you give Vitamin D to a random group of people with high blood pressure, the results are often “modest” or even “neutral.”
Now, why the discrepancy? Researchers have identified several reasons why some trials seem to “fail”:
- Firstly, the “Already Full” Tank: If a study participant already has decent Vitamin D levels, adding more won’t lower their blood pressure. So, supplements only show a dramatic effect in those who are severely deficient.
- Secondly, Dosage and Duration: Some studies used doses that were too low or didn’t last long enough to reverse years of arterial stiffness.
- Also, Genetic Variation: Some people have variations in their Vitamin D Receptor (VDR) gene, meaning their bodies don’t respond to the “sunshine vitamin” as efficiently as others.
3. The “Sweet Spot”: Recent Meta-Analyses
Additionally, when scientists pool data from dozens of studies (a Meta-Analysis), a clearer picture emerges. Also, a major analysis published in the Journal of Hypertension [6] found that Vitamin D supplementation was most effective at lowering blood pressure in:
- Firstly, patients older than 50 years.
- Secondly, those taking a dose of at least 2000 IU per day.
- Also, in individuals who were clinically deficient at the start of the study.
Therefore, observational science tells us that Vitamin D is essential for preventing high blood pressure. However, once hypertension is established, Vitamin D acts more like a “supporting actor” rather than a “solo star.” Besides, it works best when correcting a true deficiency, rather than acting as a direct replacement for blood pressure medication.
When the Link is Strong: Subgroups Who Benefit Most With Vit. D Supplementation in HTN Prevention & Management:
While Vitamin D isn’t a “one-size-fits-all” cure for high blood pressure, clinical data reveal that the connection isn’t equally strong for everyone. For certain groups of people, correcting a deficiency doesn’t just improve bone health—it can be a significant turning point in managing their cardiovascular numbers.
Research indicates that the “blood pressure-lowering” effect of Vitamin D is most pronounced in the following subgroups:
1. Firstly, the Severely Deficient:
The most consistent finding in clinical research is that Vitamin D supplementation only moves the needle on blood pressure if you are starting from a state of true deficiency (typically defined as blood levels below 20 ng/mL).
The Evidence: A study published in the Journal of Hypertension (2015) found that patients with the lowest baseline Vitamin D levels saw the most significant drops in systolic blood pressure after supplementation. So, if your levels are already sufficient, adding more Vitamin D offers “diminishing returns” for your heart [7].
2. Secondly, the Elderly (Addressing Vascular Stiffness)
As we age, our arteries naturally lose their elasticity—a condition known as arterial stiffness. Furthermore, the skin becomes less efficient at synthesizing Vitamin D from sunlight.
The Evidence: Research published in PLOS ONE indicates that Vitamin D helps reduce “Pulse Wave Velocity” (a measure of arterial stiffness) specifically in older populations. So, by helping the blood vessels remain supple, Vitamin D helps counteract the age-related rise in systolic pressure [8].
3. Thirdly, Individuals with Obesity
Vitamin D is fat-soluble, meaning it gets stored in adipose (fat) tissue. In individuals with higher body fat percentages, Vitamin D often gets “sequestered” or trapped in fat cells, making it less available for the heart and kidneys to use.
The Evidence: Clinical trials have shown that people with obesity often require 2 to 3 times higher doses of Vitamin D to achieve the same blood-pressure-lowering effects as those with a lower BMI. So, for this group, high-dose supplementation under medical supervision is often the only way to “unlock” the cardiovascular benefits [9].
4. Additionally, People with “Salt-Sensitive” Hypertension
Some people’s blood pressure is highly reactive to salt intake. This is often linked to an overactive Renin-Angiotensin System (the system we discussed in the first section).
The Evidence: Because Vitamin D acts as a “volume dial” that turns down the Renin system, it is particularly effective for people whose hypertension is driven by salt retention. A study in the American Journal of Physiology demonstrated that Vitamin D helps the kidneys process sodium more efficiently, preventing the “salt-induced” pressure spikes [10].
Hence, if you are over 50, struggling with weight, or have a lab report showing severe Vitamin D deficiency, the “Sunshine Link” to your blood pressure is likely very strong. So, for these groups, Vitamin D isn’t just a supplement—it’s a critical part of the vascular toolkit.
The Grey Areas: Why Vitamin D Isn’t a “Magic Pill” for Everyone
If the biological link is so clear, why isn’t Vitamin D the first thing every doctor prescribes for high blood pressure? This is where the science gets complicated. While we know a lack of Vitamin D can raise blood pressure, replacing it doesn’t always bring the numbers back down immediately.
Researchers call this the “Vitamin D Paradox,” and several grey areas explain why the results in human trials are often mixed.
1. Firstly, the “Structural Damage” Threshold
One of the most significant grey areas is the timing of intervention. If a person has had low Vitamin D and high blood pressure for decades, their arteries may have already undergone physical changes, such as calcification (hardening) or permanent thickening of the vessel walls.
The Reality: At this stage, while Vitamin D might help the hormonal signals, it cannot easily “undo” the structural damage to the “pipes.” Also, studies suggest that Vitamin D is far more effective at preventing the onset of hypertension than it is at reversing long-standing, chronic high blood pressure [11].
2. Secondly, the Genetics of the “Lock and Key” (VDR Polymorphism)
Now, for Vitamin D to work, it must bind to a Vitamin D Receptor (VDR)—think of the vitamin as a key and the receptor as a lock. But some people are born with slight genetic variations (polymorphisms) in their “locks.”
The Reality: So, even if these individuals take high doses of Vitamin D, their receptors don’t “catch” the hormone efficiently. Moreover, clinical trials often fail to account for this genetic diversity, leading to results where some people see a massive drop in blood pressure while others see zero change [12].
3. Thirdly, the “Missing Link” Co-Factors (Magnesium & Vitamin K2)
Importantly, Vitamin D does not work in a vacuum. To regulate blood pressure and calcium effectively, it requires “helper” nutrients.
- Firstly, Magnesium: This mineral is required to convert Vitamin D into its active form. So, if a patient is magnesium-deficient (which is common in India), Vitamin D supplements simply sit in the body, inactive.
- Secondly, Vitamin K2: While Vitamin D absorbs calcium, K2 ensures that calcium goes into the bones and not into the artery walls.
Many clinical trials only supplement Vitamin D in isolation. But without these cofactors, the cardiovascular benefits are often muted or lost entirely [13].
4. Finally, the “U-Shaped” Curve (The Question of Toxicity)
There is an ongoing debate in the medical community about whether “more is always better.”
The Reality: Some research suggests a U-shaped relationship, where both very low and excessively high levels of Vitamin D could potentially cause issues, including calcium buildup in the blood vessels (hypercalcemia), which can actually increase arterial stiffness. So, finding the “sweet spot” (usually between 30–50 ng/mL) is a grey area that varies from person to person [14].
Basically, science isn’t saying Vitamin D doesn’t work; it’s saying that Vitamin D is part of a complex “team.” If your “pipes” are already damaged, if your genetics are different, or if you’re missing “teammates” like Magnesium, the vitamin alone can’t do the heavy lifting. Yet, it has a role in preventing and managing hypertension. Besides, its deficiency can trigger HTN, such as no control on RAS to let salt be excreted and prevent the over-constriction of blood vessels.
The Difference Factor: When Hypertension Is NOT Linked to Vitamin D
It is easy to look at the research and assume that Vitamin D is the “missing link” for every high blood pressure diagnosis. However, clinical accuracy requires us to distinguish between secondary hypertension (caused by a deficiency or specific condition) and primary hypertension (caused by lifestyle, genetics, or age).
So, understanding when Vitamin D won’t help is just as important as knowing when it will. Here is when the “Sunshine Link” usually takes a backseat:
1. Firstly, Essential (Primary) Hypertension and Genetics
Now, for the vast majority of adults, high blood pressure develops gradually over many years with no single identifiable cause. Additionally, this is often driven by a combination of genetic predisposition and the natural ageing of the cardiovascular system.
The Reality: If your parents and grandparents developed hypertension in their 40s despite healthy outdoor lifestyles, your condition likely has a strong polygenic basis. So, while Vitamin D is still important for general health, it is unlikely to “override” a deep-seated genetic blueprint for high blood pressure [15].
2. Secondly, Salt-Insensitive Hypertension
In the previous section, we noted that Vitamin D helps “salt-sensitive” individuals. However, a significant portion of the population has “salt-insensitive” hypertension.
The Reality: In these cases, blood pressure does not fluctuate based on sodium intake or the Renin-Angiotensin System’s fluid regulation. Instead, the pressure is driven by Sympathetic Overactivity (the “fight or flight” nervous system). Since Vitamin D primarily targets the hormonal/kidney pathway, it has little effect on blood pressure driven by chronic stress or nervous system triggers [16].
3. Thirdly, Secondary Hypertension (The Non-Nutritional Causes) [17]
Also, sometimes, high blood pressure is a “symptom” of a different underlying medical problem. In these scenarios, Vitamin D levels are irrelevant to the blood pressure reading:
- Obstructive Sleep Apnea (OSA): If you stop breathing periodically during sleep, your brain sends a massive surge of adrenaline to wake you up, spiking your blood pressure. Also, no amount of Vitamin D can fix the mechanical airway obstruction causing the spike.
- Kidney Disease (Renal Artery Stenosis): If the physical “pipes” leading to the kidneys are narrowed, the body will spike blood pressure to ensure the kidneys get blood. Now, this is a mechanical issue that requires medical or surgical intervention.
- Adrenal Gland Tumours: Additionally, small, often benign growths can overproduce hormones like aldosterone, which can skyrocket blood pressure independently of Vitamin D status.
4. Finally, Lifestyle “Overpowers”
Even a perfect Vitamin D level cannot neutralise the vascular damage caused by certain lifestyle factors:
- High Alcohol Consumption: Firstly, alcohol directly stiffens arteries and increases heart rate.
- Smoking: Secondly, nicotine causes immediate, acute vasoconstriction (tightening of the arteries) that Vitamin D’s “relaxation” signals cannot overcome.
- High Sodium/Low Potassium Balance: Besides, if the diet is extremely high in processed salts and devoid of potassium, the cellular “pump” that regulates blood pressure remains broken regardless of vitamin status.
So, think of Vitamin D as a “fine-tuner” for your blood pressure. Now, if the “engine” of your hypertension is a genetic defect, a mechanical blockage in your kidneys, or the daily “smoke” of a cigarette habit, fine-tuning the vitamins won’t fix the breakdown.
From Lab to Life: What Should You Do Next?
Now that we’ve explored the intricate link between the “sunshine hormone” and your blood pressure, the question remains: How do you use this information to protect your heart? Transitioning from scientific theory to a personal health strategy requires a targeted approach. So, taking a random multivitamin isn’t enough; you need to ensure your body can actually use the “sunshine vitamin” you’re giving it.
1. The Testing Protocol: Know Your Numbers
Before starting any high-dose regimen, you must establish your baseline.
- The Test: Request a 25-hydroxyvitamin D [25(OH)D] blood test.
- The Target: While “normal” is often cited as 30 ng/mL, emerging cardiovascular research suggests an optimal range of 40–60 ng/mL for heart health and arterial protection [18].
2. Sunlight vs. Supplements: The Best Strategy
In a country like India, it’s a paradox that we have so much sun but such high rates of deficiency.
Sensible Sun Exposure:
Firstly, you should aim for 15–30 minutes of midday sun (between 11 AM and 2 PM) at least three times a week. At midday, UVB rays are at their peak, allowing for the most efficient Vitamin D synthesis. If you have darker skin, you may need slightly longer (up to 40 minutes) as melanin acts as a natural filter.
Furthermore, many people believe that as long as they feel “bright and warm,” their body is producing the vitamin. But, in reality, the biological process is incredibly picky about the type of light it needs. Sitting in the glass room and enjoying the sun will not help. Similarly, wearing sunscreen will do no good either if the goal is to get enough Vitamin D.
The “Filter” Problem: Why Glass and Sunscreen Block the Benefits?
Firstly, the Glass Barrier (The UVB vs. UVA Trap)
Sunlight contains two main types of ultraviolet rays: UVA and UVB.
UVB rays are the “good” rays for Vitamin D; they have the specific energy required to trigger the conversion of cholesterol in your skin into Vitamin D3. However, UVA rays have a longer wavelength and penetrate deeper (causing skin ageing and wrinkles), but they do nothing for Vitamin D production.
Most standard glass (in your car, office, or home) is designed to block UVB rays while letting UVA pass through. So, when you sit behind a glass window, you get the warmth and the potential skin damage from UVA, but your Vitamin D production remains at zero.
Secondly, the Sunscreen Paradox
Sunscreen is designed to prevent sunburn by blocking UVB rays. Because Vitamin D synthesis depends on those same UVB rays, a high-SPF sunscreen can reduce Vitamin D production by over 95% to 98%. While skin protection is vital for long-term health, “sunscreen-only” exposure means your internal “vitamin factory” never receives the signal to start working. Now, it doesn’t mean that you do not wear sunscreen, but you may not wear it while you are trying to get your body to produce Vitamin D.
Exposed Surface Area Matters
Now, your body doesn’t absorb Vitamin D through your eyes or just your face; the synthesis happens within the skin cells. So, exposing only your face and hands is rarely enough. So, to move the needle on your blood pressure and heart health, you need a larger surface area—such as the back, arms, or legs—exposed to the sun. The more skin that “sees” the sun directly, the more Vitamin D your body can manufacture in a shorter amount of time.
Clarifying the Process: The Sun is the “Spark,” Not the “Fuel”
It is a common myth that the sun “gives” us Vitamin D. In reality, the sun acts as the catalyst in a chemical factory.
Firstly, the Raw Material: Your body already has a precursor (a type of cholesterol called 7-dehydrocholesterol) sitting in your skin.
Secondly, the Spark: Now, when UVB rays hit the skin, they provide the energy to “break” a chemical bond in that cholesterol, turning it into Pre-vitamin D3.
Finally, the Refinement: Your body heat then converts that into Vitamin D3, which travels to the liver and then the kidneys to become the “active” hormone that actually helps regulate your blood pressure.
The “Safe Sun” Strategy
So, to balance heart health with skin safety, dermatologists and cardiologists often suggest:
- Short, Targeted Bursts: Firstly, 15–20 minutes of “naked” skin exposure (no sunscreen) during peak UVB hours (11 AM – 2 PM).
- The Shadow Rule: Secondly, if your shadow is longer than you are, the sun is too low in the sky for the atmosphere to let enough UVB rays through.
- Protection After Production: Thirdly, once you’ve had your 20 minutes, apply sunscreen or move to the shade to prevent skin damage.
The Supplement Shift:
Finally, if you work indoors or live in a highly polluted city, sun exposure may be insufficient. Clinical guidelines often recommend 2,000–4,000 IU of Vitamin D3 daily for those with hypertension and proven deficiency [19].
So, when sunshine is not on your cards, it is beneficial to shift on supplements. However, you need to have some diagnostic tests before starting any supplement. Furthermore, supplementation should be only after a thorough discussion with your doctor. Do not start or stop any medicine unless advised by a registered medical practitioner or a healthcare professional.
3. The “Co-Factor” Secret: Magnesium and Vitamin K2
Vitamin D is a team player. To lower blood pressure effectively, it needs two critical partners, Magnesium and Vitamin K2 (MK 7), as discussed earlier [20].
4. Precautions: The “U-Shaped” Warning
More is not always better. Excessive Vitamin D (typically from extremely high-dose supplements over 10,000 IU daily without supervision) can lead to hypercalcemia, where too much calcium in the blood actually causes heart rhythm issues and kidney stones.
Action Step: So, always re-test your levels after 3 months of supplementation to ensure you stay in the “Goldilocks zone” (not too low, not too high).
Finally, don’t treat Vitamin D like a magic pill; treat it like a lifestyle adjustment. Rather, get your blood tested, spend a few minutes in the midday sun, and ensure your diet includes magnesium-rich foods (like nuts and leafy greens) or a balanced co-supplement.
Summary Checklist for Your Next Doctor’s Visit:
- Firstly, ask for a 25(OH)D test.
- Secondly, discuss a target level of 40–60 ng/mL.
- Thirdly, ask if a Vitamin D3 + K2 combination is right for your cardiovascular profile.
- Finally, check your Magnesium status if your Vitamin D levels aren’t rising as expected.
A New Pillar in Heart Health
For years, we viewed Vitamin D as a secondary nutrient—something for bones, but a “nice-to-have” for everything else. Today, science is rewriting that narrative. The “Sunshine Hormone” is a vital regulator of your cardiovascular system, acting as a natural brake on the hormones that spike blood pressure and a protective shield for the lining of your arteries.
However, the most important takeaway is that Vitamin D is not a replacement for traditional hypertension management; it is a powerful partner. While it may not override a genetic predisposition or fix a kidney obstruction, it can significantly lower the “baseline” pressure for those who are deficient, elderly, or struggling with salt sensitivity.
In the fast-paced, indoor world we live in—especially in urban India—the “Sunshine Link” is often the most neglected part of the heart health puzzle. So, by checking your levels, ensuring you have the right “teammates” like Magnesium and K2, and getting sensible sun exposure, you are doing more than just taking a vitamin. Additionally, you are giving your heart the biological environment it needs to beat steadily and stay supple.
Your Next Step
Don’t guess—test. So, the next time you visit your doctor for a blood pressure check, ask to add a Vitamin D test to your panel. It is a simple, low-cost step that could provide the missing piece in your journey toward a healthier heart.
Partner in Health: Help Us Bridge the Gap in Cardiac Care
As we have explored in this post, the prevalence of hypertension and Vitamin D deficiency in India is reaching critical levels. The science is clear, but the solution requires more than just knowledge—it requires access.
At Best Biotech and our dedicated cardiac division, Best Cardia, we believe that world-class treatment shouldn’t be a luxury. From the T-Star range for blood pressure management to Redivit Gold and Diabest for essential metabolic support, our goal is to ensure that high-quality, affordable therapeutics are available in every district and town across the nation.
Now, this is where you come in.
We are actively seeking passionate partners to join us in this mission. So, we are opening opportunities for Pharma PCD (Propaganda Cum Distribution) and Pharma Franchise collaborations for professionals who understand the value of ethical healthcare.
This is not just a commercial venture; it is an opportunity to be the bridge between clinical excellence and the patients who need it most. By partnering with us, you gain:
A Complete Cardiac & Diabetic Range:
Firstly, you get access to our comprehensive portfolio (General Physician medicines, gynaecology medicines in Dydrobest division, respiratory care medicines in Inspicare, anti-diabetics, ortho care, wound care, ophthalmologic care in Jicky Eyes, cosmetics in Defrent and others, including the advanced formulations listed below.
Vitamin D Supplements & Hypertension Management Medicines available for Pharma Marketing:
| Brand Name | Composition | Impact |
| REDIVIT GOLD-CD3 TAB | Methylcobalamin 1500mcg + Alpha Lipoic Acid 100mg + Inositol 100mg + Folic Acid 1.5mg + Pyridoxine 100mg + Vitamin D3 (1,000 I.U) + Chromium Picolinate + Calcium Carbonate + Benfotiamine | A comprehensive nerve and bone support supplement. The 1,000 I.U. of Vitamin D3 supports calcium absorption and cardiovascular health, while the B-vitamins and Alpha Lipoic Acid help protect nerves (often useful for hypertensive patients with diabetes). |
| DIABEST Capsules | Fenugreek + Costus Igneus + Gymnema + Banana Leaf + Cholecalciferol (Vitamin D3) 600 I.U. + Magnesium 20 mg + Chromium + Vitamins C & E | Primarily for metabolic support and blood sugar control. Contains Vitamin D3 and Magnesium, which are the exact “co-factors” mentioned in our blog post for regulating blood pressure naturally. |
| DIABEST Sachets | (Comprehensive Blend including Green Tea, CoQ10, Resveratrol, Omega-3s) + Cholecalciferol (Vitamin D3) 600 I.U + Magnesium 100mg | A high-potency antioxidant and metabolic support sachet. Includes heart-healthy ingredients like Resveratrol and EPA/DHA, along with Vitamin D for vascular health. |
| SACARDIA-50 TABLET | Sacubitril 24 mg + Valsartan 26 mg | A potent combination (ARNI class) used to treat heart failure and manage resistant hypertension. It relaxes blood vessels and reduces fluid retention. |
| TSTAR-20 Tablets | Telmisartan 20mg | An Angiotensin Receptor Blocker (ARB). It blocks the “tightening” signal in blood vessels, lowering blood pressure effectively. |
| TSTAR-40 Tablets | Telmisartan 40mg | A higher strength standard dosage for blood pressure management. |
| T-STAR-CL Tab | Telmisartan 40 mg + Cilnidipine 10 mg | A dual-action combination. Telmisartan relaxes vessels via hormone blocking, while Cilnidipine (a Calcium Channel Blocker) relaxes vessels by blocking calcium uptake. |
| T-STAR-CT TAB | Telmisartan 40 mg + Chlorthalidone 12.5mg | Combines a BP medication with a Diuretic (water pill). Useful for patients who retain salt/fluid, helping reduce pressure volume. |
| T-STAR-H TAB | Telmisartan 40 mg + Hydrochlorothiazide 12.5 mg | Another common combination of an ARB and a Diuretic (HCTZ) to manage moderate to severe high blood pressure. |
| T-STAR-MCL-25 Tab | Telmisartan 40mg + Metoprolol 25mg + Cilnidipine 10mg | A powerful Triple Combination. It targets three mechanisms: hormone blocking (Telmisartan), heart rate control (Metoprolol/Beta-blocker), and vessel relaxation (Cilnidipine). Used for difficult-to-control BP. |
Quality You Can Trust:
Since Best Biotech is an ISO 9001:2015 certified company, we prioritise efficacy and safety in every batch.
Monopoly Rights:
Finally, we believe in empowering our partners to grow their business in their specific regions without saturation. So, if you are a pharma professional, distributor, or entrepreneur looking for a meaningful business opportunity that combines steady growth with the satisfaction of making healthcare accessible, we invite you to start a conversation with us.
Let’s grow together while keeping India’s heart healthy.
Contact us today to discuss franchise availability in your region.
Quick Links:
- Best Cardia Division Products
- Once a Week Medicine for Diabetes: WIKLYONE (Trelagliptin): How it Works?
- Struggling with the Mucus and Wheeze of COPD? Why Targeting Both Can Be a Game Changer
- Why Pharma Exhibitions Matter: 9 Top Reasons to Attend Next Pharma Expo
- Why Your Acid Reflux is Not Improving With Medicines? What Can Be Done?
References:
- Li, Y. C., et al. (2002). “Vitamin D: A negative endocrine regulator of the renin-angiotensin system.” Journal of Clinical Investigation.
- Molinari, C., et al. (2011). “Vitamin D activation of endothelial nitric oxide synthase.” Cardiovascular Research.
- Scragg, R., et al. (2007). “Serum 25-hydroxyvitamin D, antihypertensive medication, and blood pressure in the Third National Health and Nutrition Examination Survey.” American Journal of Hypertension.
- Wang, T. J., et al. (2008). “Vitamin D deficiency and risk of cardiovascular disease.” Circulation.
- Vimaleswaran, K. S., et al. (2014). “Association of vitamin D status with arterial blood pressure and hypertension risk: a mendelian randomisation study.” The Lancet Diabetes & Endocrinology.
- Qi, D., et al. (2017). “Vitamin D supplementation and blood pressure in Type 2 Diabetes: A meta-analysis of randomised controlled trials.” Journal of Hypertension.
- Chen, L., et al. (2015). “Effect of Vitamin D supplementation on blood pressure: a systematic review and meta-analysis.” Journal of Hypertension.
- Geng, J., et al. (2015). “The influence of Vitamin D supplementation on arterial stiffness: A meta-analysis of randomised controlled trials.” PLOS ONE.
- Ekwaru, J. P., et al. (2014). “The importance of body weight for the dose-response relationship of oral Vitamin D supplementation.” PLOS ONE.
- Forman, J. P., et al. (2010). “Effect of Vitamin D on Endothelial Function and the Renin-Angiotensin System.” American Journal of Physiology.
- Pilz, S., et al. (2009). “Vitamin D and cardiovascular disease: state of the evidence.” Trends in Cardiovascular Medicine.
- Pan, W. H., et al. (2009). “Vitamin D receptor gene polymorphisms and hypertension.” Journal of Human Hypertension.
- Uwitonze, A. M., & Razzaque, M. S. (2018). “Role of Magnesium in Vitamin D Activation and Function.” The Journal of the American Osteopathic Association.
- Durup, D., et al. (2012). “A Reverse J-Shaped Association of Serum 25-Hydroxyvitamin D with Total Mortality.” The Journal of Clinical Endocrinology & Metabolism.
- Kotchen, T. A. (2011). “Genetic Determinants of Hypertension.” Hypertension.
- Sanada, H., et al. (2011). “The sympathetic nervous system and hypertension.” Current Hypertension Reports.
- Rimoldi, S. F., et al. (2014). “Secondary arterial hypertension: when, who, and how to screen?” European Heart Journal.
- Journal of the Endocrine Society (2021) notes that cardiovascular benefits are most pronounced when levels are maintained consistently above the “insufficiency” threshold of 30 ng/mL.
- Mayo Clinic (2024) and The Endocrine Society recommend these ranges to avoid toxicity while ensuring vascular benefit.
- The Journal of the American Osteopathic Association (2018) highlights that Magnesium is essential for Vitamin D metabolism and that its absence can render supplementation ineffective.